Motor unit number estimation & spinal muscular atrophy
Monitoring disease & treatments with QtracW & MScanFit
In a recent study published in the European Journal of Neurology (Schneider et al. 2021), Christian Schneider and colleagues at the University Hospital of Cologne and Research Center Jülich used motor unit number estimation (MUNE) and MScanFit software to examine the organization and short-term changes of motor units in adult nusinersin-treated patients suffering from Spinal Muscular Atrophy (SMA). Comparisons were made with age-matched healthy control subjects and patients with amyotrophic lateral sclerosis (ALS), where the use of MUNE/MScanFit is well established (Jasobsen et al. 2017).
What is Spinal Muscular Atrophy and how is it treated?
Spinal Muscular Atrophy or SMA is an incurable heterogenic motor neuron disease caused by a homozygous disruption of the SMN1 gene on chromosome 5q. The disease, which is phenotypically subdivided into types 1-4, is characterised by a progressive loss of motor function.
Limited treatments for SMA include gene replacement therapy, involving a single infusion of SMN1 gene or the drug nusinersin (Spinraza), a synthetic anti-sense oligonucleotide that enhances splicing of the Survival Motor Neuron SMN2 gene, thereby boosting levels of survival motor neuron protein, critical for the development of healthy motor neurons.
Nusinersin was approved by the FDA in 2018/19 and is widely used to treat SMA in children and infants, but very little is known about its benefits or effects in adults, especially in terms of electrophysiological measurements of motor function. Previous studies have examined motor unit changes in children, in response to nusinersin treatment (Schneider and colleagues aimed to investigate whether nusinersin could be of benefit to adults with SMA.
Motor unit estimation used threshold tracking hardware and software available from Digitimer
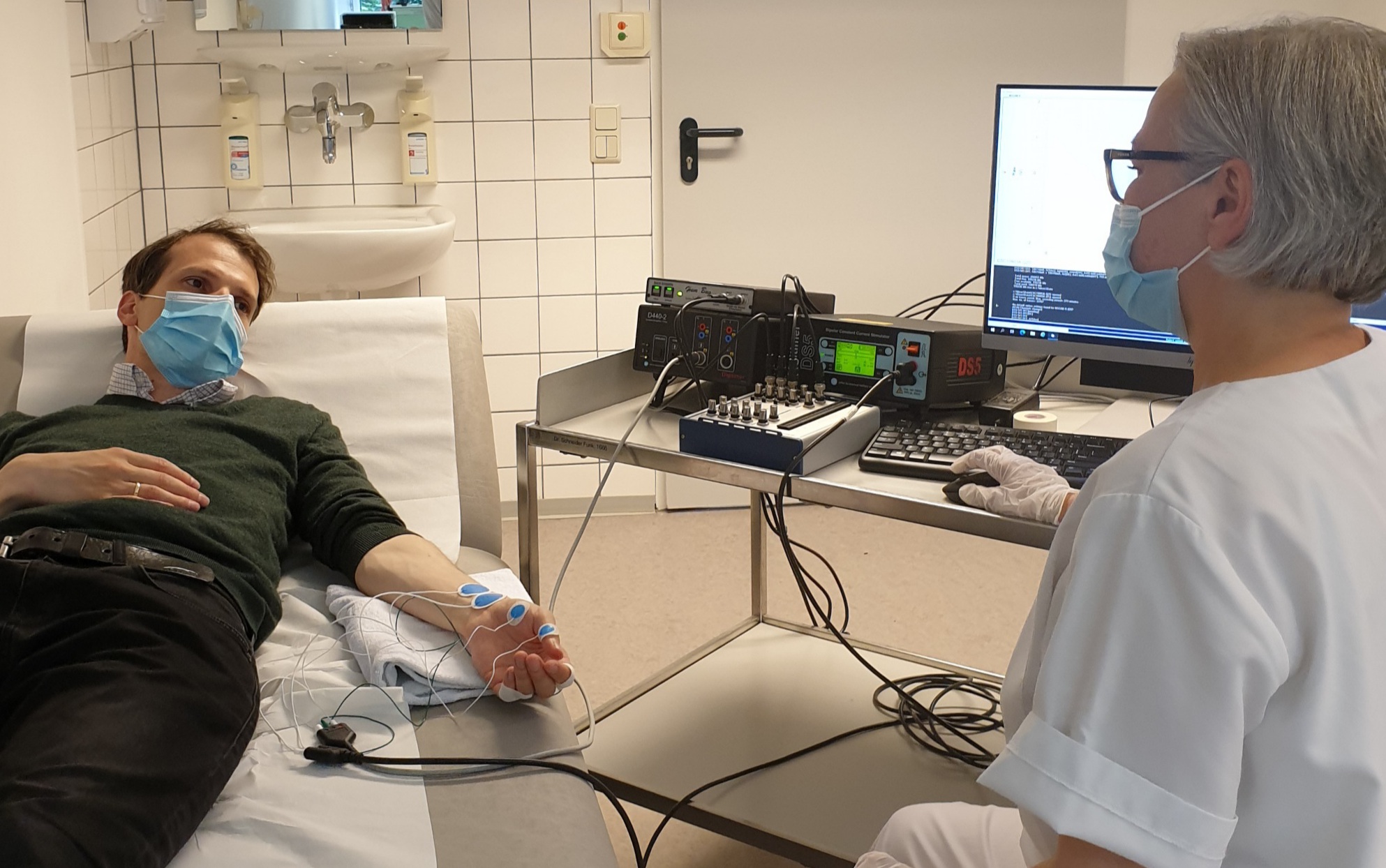
In order to assess motor unit changes, the group used motor unit number estimation (MUNE) methods. Briefly, this involved electrical stimulation of the median nerve, with recordings of compound muscle action potentials (CMAP) being taken from the abductor brevis muscle. Constant current stimulation was delivered by the Digitimer DS5 Bipolar Constant Current Stimulator and recordings were made via our D440 Isolated EMG Amplifier. A Quest Scientific Humbug was also employed to remove 50Hz interference, which is sometimes an issue in electrically noisy hospital environments or when using a mobile recording setup.

CMAP recordings were acquired using QtracW threshold tracking software developed by Prof. Hugh Bostock and available exclusively from Digitimer. EMG responses were fed back to QtracW via a National Instruments data acquisition interface (USB-6341-BNC), which was also used to automatically control the stimulation pulses from the DS5.
Finally, MUNE analysis was made possible through MScanFit, which is a freeware component within the QtracW software. Fitting of CMAP data allowed the researchers to obtain the following measures of motor function:-
- MscPeak – the maximum CMAP amplitude.
- MSFNUnits – the estimated number of motor units.
- MscD50 – a value that represents the number of CMAP scan discontinuities, which when summed, exceed 50% of the CMAP amplitude.
- MSFMeanUnitAmp – the mean amplitude of single motor unit potentials.
- MSFLargestAmp – the amplitude of the largest motor unit potential.
- MSFMedianAmp – the median of the amplitudes of single motor unit potentials expressed as a percentage of CMAP.
MScanFit analysis indicated that nusinersin may be of use in adults with mild SMA
The parameters detailed above gave the authors comprehensive information relating to motor unit changes under two pathophysiological conditions and in response to nusinersin treatment. While SMA patients typically exhibit loss of motor units in distal muscles, when compared to the control group, their CMAP amplitudes were maintained, probably as a result of collateral sprouting.
Results also suggested that adults with milder SMA symptoms may benefit from nusinersin treatment via the recovery of smaller motor units. The study further demonstrated that QtracW and MScanFit may be powerful research tools for disease and/or treatment monitoring, especially as they revealed subtle changes that standard electrodiagnostic tests would be incapable of detecting.
Want to find out more?
If you have an interest in studying motor units and would like to discuss the equipment and software requirement, please do not hesitate to contact our team at Digitimer or our local representative. A recent review (Tankisi, 2021) has also summarised the pathologies that have already been investigated with MScanFit and provides further detail relating to the advantages MScanFit offers over the other MUNE methodology. Finally, if you would like to learn more about Dr Schneider’s research, you can read the open-access paper via the European Journal of Neurology website.
We thank Dr Christian Schneider for allowing us to use several photographs, but this contribution is not intended to endorse any of the hardware or software products/brands mentioned in this article.
Further Reading
- A.B. Jacobsen, H. Bostock, A. Fuglsang-Frederiksen, L. Duez, S. Beniczky, A.T. Møller, J.U. Blicher, H. Tankisi, Reproducibility, and sensitivity to motor unit loss in amyotrophic lateral sclerosis, of a novel MUNE method: MScanFit MUNE, Clinical Neurophysiology, Volume 128, Issue 7, 2017, Pages 1380-1388, ISSN 1388-2457, https://doi.org/10.1016/j.clinph.2017.03.045.
- , et al, Motor unit changes in children with symptomatic spinal muscular atrophy treated with nusinersen,
- Tankisi H. MScanFit motor unit number estimation: A novel method for clinics and research. Neurol Sci Neurophysiol [serial online] 2021 [cited 2021 Aug 6];38:1-5. Available from: http://www.nsnjournal.org/text.asp?2021/38/1/1/311966


